
Arrive at the correct procedure code by breaking down the operative report.
Even seasoned coding professionals occasionally find it challenging to assign the appropriate ICD-10-PCS codes from the operative report. Mastering the procedural coding system used in the inpatient hospital setting takes practice. Medical coders reporting inpatient services should start by reading the operative report, which tells the patient’s story, and then break down the procedure step by step.
Doing so helps build the ICD-10-PCS code accurately, improves productivity, and enhances coding quality. Read on to see what this process entails.
ICD-10-PCS Structure
There is a reliable process for constructing the codes in ICD-10-PCS. The distinct letters and numbers are referred to as values. They are selected and arranged to occupy the seven spaces of the code, known as characters.
Values
Out of 26 letters, 24 letters are used to build a code. The letters I and O are the exceptions; they’re not used because they are easily confused with the numbers one and zero.
Characters
All ICD-10-PCS codes are seven characters in length, and each of the seven characters represents an aspect of the procedure. Below are the seven characters that make up an ICD-10-PCS code:
- 1st character is Section
- 2nd character is Body System
- 3rd character is Root Operation
- 4th character is Body Part
- 5th character is Approach
- 6th character is Device
- 7th character is Qualifier
Let’s go though some case scenarios to demonstrate how to arrive at the correct ICD-10-PCS code.
Put Your Coding Skills to the Test
To help you better understand what this process involves, here are two examples to demonstrate proper procedural coding; one is a surgical procedure and the other is a non-surgical procedure.
Surgical Procedure
Operative Report
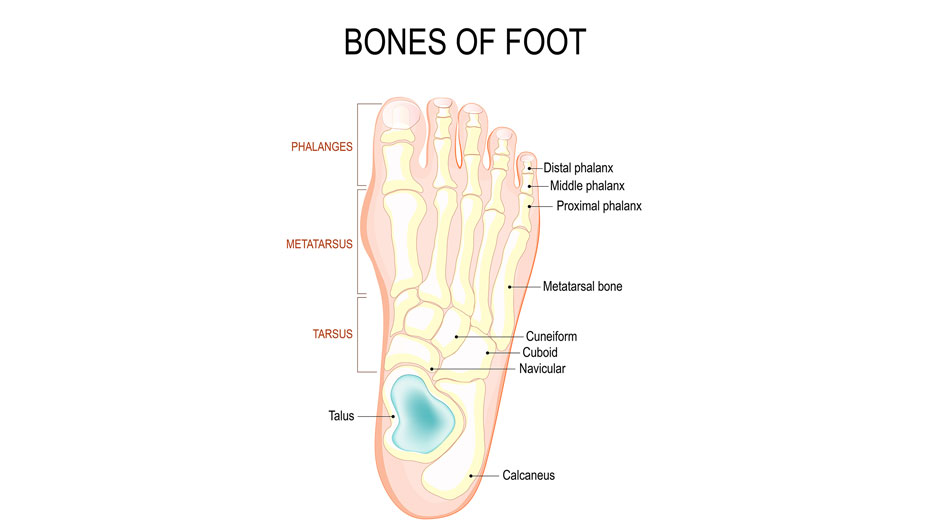
- Pre-operative diagnosis: Uncontrolled diabetes; osteomyelitis distal and middle phalanx, second toe, left foot
- Post-operative diagnosis: Uncontrolled diabetes; Osteomyelitis distal and middle phalanx, second toe,
left foot
Type of anesthesia administered: Local with IV sedation
Procedure performed: Amputation of distal and middle phalanx of the second toe of left foot
Description of procedure
The patient was taken to the operating room and placed in the supine position. After IV sedation, an ankle block of 20 mL of 1% lidocaine plain was instilled on the left ankle. The patient was prepped and draped in the usual aseptic manner. The fish mouth incision surrounding the proximal interphalangeal joint of the second toe of the left foot was made and carefully deepened down to the level of bone. Distal and middle phalanx were disarticulated through the proximal interphalangeal joint of the second toe of the left foot. All bleeding vessels were cauterized. It was irrigated with copious amounts of sterile saline and inspected for any remaining debris of which none was found. Skin closed with 3-0 nylon in a simple interrupted suture fashion. Dressings of xeroform, fluffs, kerlix, and ace wrap were placed. The patient tolerated the procedure well and was transferred to the post-acute care unit with vital signs stable.
Stories facilitate solidifying abstract ideas and interpreting complicated messages. Let’s read this procedure report like a story by asking the usual questions: why, where, what, and how? Jot things down as you go. The patient’s story goes like this:
The patient presented to the hospital with uncontrolled diabetes and osteomyelitis of the distal and middle phalanx, second toe, left foot. In the operating room, a fish mouth incision was made, and the surgeon performed disarticulation of the distal and middle phalanx through the proximal interphalangeal joint of the second toe on the left foot.
When building an ICD-10-PCS code, always start with “why?” Identify the purpose, intent, or objective of the procedure performed. Once you know why the procedure was performed, you can understand the whole procedure and the rest your decisions will fall into place.
Why – This is the reason/explanation of the procedure: disarticulation or amputation due to uncontrolled diabetic osteomyelitis
Where – The site/location of the procedure: second toe, left foot
How – The approach: incision
What – The name of the surgical procedure: amputation of distal and middle phalanx of the second toe on the left foot
Let’s go step by step through the procedure, following the applicable rules or instructions:
1. Find the main term in the index.
2. Determine the root operation.
3. Follow the direction of the index and choose the three-character table.
4. After locating the table, select the characters four to seven.
5. Find the body part.
6. Identify the approach.
7. Check whether or not a device was used.
8. Confirm whether a qualifier was present.
9. Finalize the seven characters of the ICD-10-PCS code.
In this case scenario, there are two qualifiers, hence, two ICD-10-PCS codes:
1. Look up Disarticulation.
2. This directs us to see Detachment.
3. Under Detachment, find the sub term Toe.
4. Under Toe, locate the sub term 2nd.
5. Under 2nd, find the sub term Left.
6. You are directed to 0Y6S0Z.
7. Go to the Tabular List.
8. For the first code, select qualifier 2 for Mid.
9. For the second code, select qualifier 3 for Low.
The final code is:
0Y6S0Z2 Detachment at Left 2nd Toe, Mid, Open Approach
We start by dividing the first part of the procedure note into a story and then we find the key terms and combine them to build the right ICD-10-PCS code.
Non-surgical Procedure
Now let’s practice coding a non-surgical procedure.
Operative Report
- Pre-operative diagnosis: Breast cancer
- Post-operative diagnosis: Breast cancer
- Procedure performed: Port-a-cath placement
Description of procedure
The patient was taken to the operating room and placed in the supine position. The right chest and neck were prepped and draped in the sterile fashion, and 20 cc of 1% Lidocaine was injected. The right subclavian vein was punctured, and a wire was passed into the superior vena cava. An introducer kit was introduced into the subclavian vein, and a port-a-cath was placed through the introducer, and fluoroscopy was placed down to the superior vena cava. The pocket was then made over the right pectoralis major muscle superior to the breast and the port-a-cath receptacle was placed into this pocket and tacked down. The catheter was then tunneled through to this receptacle. Hemostasis was achieved, and the subcutaneous tissue was closed with # 2-0 dexon. The skin was closed with #3-0 nylon. The port-a-cath was flushed with saline.
The story of the patient’s condition goes like this:
The patient with breast cancer presented to the hospital for insertion of a port-a-cath device for use in chemotherapy. In the operating room, two devices were inserted using two different approaches: A port-a-cath device was inserted into the superior vena cava via a percutaneous approach, and a vascular access device was inserted through the subcutaneous tissue and fascia of the chest via an open approach.
Why – The reason/explanation of the procedure was because the patient had breast cancer and devices were inserted.
Where – The site/location of the procedure was the superior vena cava and chest.
How – The approach was percutaneous.
What – The name of the surgical procedure is insertion of port-a cath device.
In this case scenario, two devices were inserted using two different approaches, hence, there are two ICD-10-PCS codes.
The first is an infusion device inserted into the superior vena cava through a percutaneous approach.
1. In the index, locate the main term Insertion of device in.
2. Find the sub term Vena Cava.
3. Locate sub term Superior, which directs you to 02HV.
4. Go to the Tabular List.
5. Select 3 for Percutaneous approach.
6. Select 3 for Infusion device.
7. Select Z for No Qualifier.
The final code is:
02HV33Z Insertion of Infusion Device into Superior Vena Cava, Percutaneous Approach
The steps for determining the code for the second procedure are as follows:
1. In the index, locate the main term Insertion of device in.
2. Find the sub term Subcutaneous Tissue and Fascia.
3. Find the sub term Chest, which directs you to 0JH6.
4. Go to the Tabular List.
5. Select 0 for the Open approach.
6. Select W for Vascular Access Device, Totally Implantable.
7. Select Z for No Qualifier.
The final code is:
0JH60WZ Insertion of Totally Implantable Vascular Access Device into Chest Subcutaneous Tissue and Fascia, Open Approach
We can expect accurate results as long as we follow the rules outlined above and complete the steps in the correct order.
Be a Problem, Solver
Critical thinking skills are a must for coding professionals to increase productivity and enhance quality. Possessing these skills permits us to be actively engaged in learning and facilitates success. Being able to compose stories and break them down using a step-by-step process helps in building ICD-10-PCS codes and keeps us enjoying the learning process. Never stop learning and have fun!
For More Information: 84869 how to build icd 10 pcs codes from op reports